Disclaimer: I’m pro-LC (P<0.05), but not anti-LF because LF works better than LC for some people. And with the exception of things like keto for neurological issues, I think macros take a back seat to many other factors.
Myths: carbs cause insulin resistance (IR), diabetes, and metabolic syndrome. Carbs are intrinsically pathogenic. If a healthy person eats carbs, eventually they’ll get sick.
And the only prescription is more keto.
And of course all of this could’ve been prevented if they keto’d from the get-go.
Proponents of these myths are referring to regular food carbs, not limited to things like Oreo Coolattas (which would be more acceptable, imo). Taubes, Lustig, Attia, and many others have backed away from their anti-carb positions, yet the new brigade proceeds and has even upped the ante to include starvation. Because “LC = effortless fasting?”
Does this sound sane?
“No carbs ever,
no food often…
otherwise diabetes.”
no one in their right mind would say lentils & beans cause diabetes
Recent comments about FASTER have upgraded this study to “the only long-term study on fat-adaptation.” Needless to say, I disagree. Again.
Side note: FASTER had no randomization or intervention (ie, confounded by selection bias, among others); they basically recruited long-term low carb & high carb ultra-endurance runners and measured the stuffings out of ’em.
Ultimately, they showed a very high maximal fat oxidation rate in low carb ultra-runners, 1.5 grams per minute. This is important because MAXIMAL HUMAN FAT BURNING CAPACITY
In previous studies on SAD (Standard Athletic Diet haha), maximal fat oxidation at similar VO2max% has been reported to be much lower, <1 g/min (eg, Hetlid et al., 2015 and Volek et al., 2016).
I came across a recent study on a mouse model of Angelman Syndrome (an epigenetic disorder), and wasn’t surprised to learn there’s a strong circadian component to it. Epigenetics are one of the main ways circadian rhythms are programmed.
In this case, the circadian connection is more direct.
Angelman Syndrome (AS): you inherit 2 pairs of each gene, one from Mom and one from Dad. In some cases, one of the copies is silenced via epigenetics and you’re basically just hoping the other one is in good shape. In the genetically relevant region in AS, the paternal copy is silenced and the maternal copy does all the heavy lifting, but in AS, the maternal copy is mutated or absent, so none of the genes in this region are expressed.
Interestingly, scientists found that one of the genes, Ube3a (an ubiquitin ligase), is involved in regulating Bmal1, a core circadian gene (Shi et al., 2015) . And mice with a silenced paternal Ube3a and mutant maternal Ube3a exhibit many of the same circadian symptoms of children with AS. They don’t mimic all of the symptoms as there are many other genes in this region. But both show circadian abnormalities.
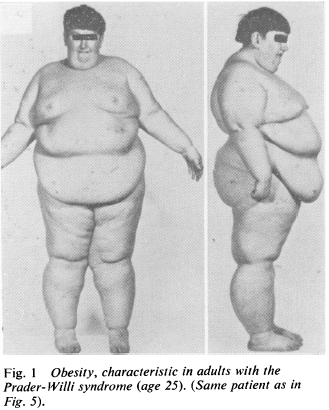
Prader-Willi Syndrome (PWS) is the epigenetic opposite: same region of DNA, but silenced maternal copy and mutant or absent paternal copy. This disorder is characterized by massive obesity and low muscle mass (among other things).
While reading about this disorder, I was taken aback with how the obesity was explained.
“Insatiable appetite” (Laurance et al., 1981), although from what I can gather, these children would develop massive obesity even if they were fed cardboard. Some studies even showed no change in food intake and/or energy expenditure (eg, Schoeller et al., 1988), which led some researchers to publish entire papers about how these children must be lying and/or stealing food (eg, Page et al., 1983) .
Further, other researchers even explained their obesity was due to an inability to vomit (Butler et al., 2007).
THEY’RE OBESE BECAUSE THEY’RE NOT BULEMIC.
AYFKM?
When these kids gain weight, it’s nearly all fat mass; when they lose weight, it’s nearly all muscle [shoulda been a BIG hint]… this even led some researchers (who detected no change in fat mass after significant weight loss) to conclude that their techniques to assess body composition must not be valid in this population because: surely, they must’ve lost some fat mass like normal people do.
THEY FAILED TO CONSIDER THIS IS AN EXTREME CIRCADIAN MISMATCH DISORDER IN NUTRIENT PARTITIONING
It was actually painful to read: these kids are being accused of stealing food and not vomiting because that’s the only way to explain it.
NO IT’S NOT, SCIENCE.
They can be forced into losing fat while maintaining some muscle with an extreme protein-sparing modified fast (eg, Bistrian et al., 1977)…
A few research groups have considered the possibility it’s a hormonal disorder, and some fairly long-term studies with GH replacement have shown promising results (eg, Carrel et al., 1999).
Prader-Willi Food Pyramid. Wait, wut? O_o
Some have even speculated involvement of leptin (eg, Cento et al., 1999), although this hasn’t been followed-up on.
Disclaimer: I don’t know the cure or best treatment modality for Prader-Willi, although given the strong circadian component in its sister condition, Angelman’s Syndrome, I strongly believe this avenue should be explored (in combination with the seemingly necessary hormonal corrections, which have been the only successful interventions yet). “Diet” doesn’t work; these kids aren’t obese because they’re stealing food or failing to vomit. Interventions strictly targeting CICO have massively failed this population.
Side note: in the Angelman Syndrome mouse model, *unsilencing* the paternal copy worked… maybe the same could work in PWS (and/or other forms of obesity)…?
Evidence supporting potential circadian-related treatment modalities for PWS:
A Prader-Willi locus IncRNA cloud modulates diurnal genes and energy expenditure (Powell et al., 2013)
Magel2, a Prader-Willi syndrome candidate gene, modulates the activities of circadian rhythm proteins in cultured cells (Devos et al., 2011)
Circadian fluctuation of plasma melatonin in Prader-Willi’s syndrome and obesity (Willig et al., 1986)
And the connection with LIGHT:
Artificial light at night: melatonin as a mediator between the environment and the epigenome (Haim and Zubidat, 2015)
Circadian behavior is light re-programmed by plastic DNA methylation (Azzi et al., 2014)
PWS is much worse than just nutrient partitioning (seriously, just spend a few minutes on any Prader-Willi support forum or this; maybe it is an appetite disorder, but given the data on weight gain [mostly fat mass] and weight loss [mostly muscle mass], it seems far more likely a circadian disorder of nutrient partitioning),
but that component jumped out at me; more specifically, despite the only positive results coming from non-dietary interventions, researchers were still all “#CICO.”
“Lean meat, sugar-free Jello, and skim milk”
FFS
Circadian biology, hormone replacement [where appropriate], and figure out if any specific diets help. PMSF/CR doesn’t work unless “refrigerators and cabinet pantries are locked shut.”
Maybe this applies to other forms of obesity, too.
Maybe.
Check out my Patreon campaign! Join the community of over 300 members for up-to-date information about a variety of topics in the health & optimizing wellness space. At 5 bucks a month, can’t beat it!
Affiliate links: KetoLogic for keto-friendly shakes, creamers, snacks, etc. And get 15% off your ketone measuring supplies HERE.
Still looking for a pair of hot blue blockers? TrueDarkis offering 10% off HERE and Spectra479is offering 15% off HERE. If you have no idea what I’m talking about, read this then this.
If you want the benefits of ‘shrooms but don’t like eating them, Real Mushrooms makes great extracts. 10% off with coupon code LAGAKOS. I recommend Lion’s Mane for the brain and Reishi for everything else.
Dietary protein “requirements” are some of the most context-dependent nutrient levels to decipher, and depend largely on energy balance and even meal frequency.
This wasn’t well-received in social media because bro-science & many low carb advocates say grazing is no longer in vogue — “it’s much better/healthier/whatever to eat once or twice daily, because intermittent fasting and all that jazz” …however, this may be problematic when it comes to meeting overall protein needs, which is particularly important when you’re losing weight.
@CaloriesProper Really? Drawing conclusions based on a 2 week study of 11 pts?
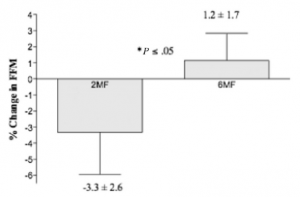
Conclusion: “On average, fat-free mass (FFM) decreased by -3.3% following the 2 meals/d condition and, on average, and increased by 1.2% following the 6 meals/d condition (P<.05).”
In other words, 6 meals per day was better for body composition than 2 meals per day. But context is everything, and this hypothesis has been tested from a variety of different angles, so what does it mean?
The relevant context here: 1) big energy deficit (1200 kcal/d for obese women is a pretty low calorie intake); and 2) “adequateTM” protein intake (75 g/d).
The standard dogma says that in the context of an adequate protein hypocaloric diet, meal frequency matters a LOT, whereas with high protein, it doesn’t matter as much. Theory being that with an “adequate” (read: too low?) overall protein intake, the fasting periods are simply too long with only two meals per day; you need either: 1) higher protein intake; 2) increased meal frequency; or 3) more calories (ie, smaller energy deficit).
In this study, BOTH diets suppressed insulin and induced weight loss, but the increased protein feeding frequency skewed the weight loss to body fat while preserving fat-free mass. I actually agree with a lot of the bro-science in this case, and also think that 75 grams of protein is not enough in the context of a big energy deficit (if body composition is a goal).
Relevant context: 6 vs. 3 meals per day (3 meals per day may not seem like that many more than 2, but it significantly cuts down on the duration of time spent with no food or protein).
Smaller energy deficit: 1700 kcal/d in overweight patients is less of a deficit than 1200 kcal/d in obese patients.
Higher protein intake: 106 – 115g/d.
Result: nitrogen balance (a surrogate for the maintenance of muscle mass) and fat loss were similar in both groups. This study fixed two problems in the abovementioned study: 1) 3 meals is better than 2 in the context of an energy deficit; and 2) protein intake was higher.
And again here, with 3 vs. 6 meals per day (Cameron et al., 2010), just to make the point that 3 meals per day is better than 2 for preserving lean mass in the context of an energy deficit.
This study tested the opposite extremes: super-low calorie intake (800 kcal/d), much lower protein intakes (20g – 30g/d), and 1 vs. 5 meals per day.
Result: “a diet with a high-protein concentration, fed as frequent small meals, is associated with better preservation of lean tissue than an isoenergetic diet with lower-protein concentration fed as fewer meals.”
1 vs. 4 meals per day; and 70 grams of protein but no energy deficit (~2000 kcal/d isn’t very hypocaloric for lean young women). In this study, no effect of meal frequency was seen, likely because 70 grams of protein isn’t inadequate when energy intake isn’t restricted.
If you’re losing weight (ie, in an energy deficit), then intermittent fasting is cool if protein intake is high (above “adequateTM“)… the bigger the energy deficit, the more protein is necessary to optimize changes in body composition.
How much is ‘enough?’ Sorry, can’t give you a gram or even gram per pound of body weight answer… but if you’re losing weight and seeing no discernible effect on body composition (muscle vs. fat mass), then it may be prudent to consider eating more protein-rich foods… and paying more attention to sleep quality (which also greatly impacts nutrient partitioning).
Affiliate links: KetoLogic for keto-friendly shakes, creamers, snacks, etc. And get 15% off your ketone measuring supplies HERE.
Still looking for a pair of hot blue blockers? TrueDarkis offering 10% off HERE and Spectra479is offering 15% off HERE. If you have no idea what I’m talking about, read this then this.
If you want the benefits of ‘shrooms but don’t like eating them, Real Mushrooms makes great extracts. 10% off with coupon code LAGAKOS. I recommend Lion’s Mane for the brain and Reishi for everything else.
Brief refresher: skeletal muscle insulin sensitivity is higher in the morning than in the evening. Exercise boosts insulin sensitivity selectively in muscle, which is relatively more important in the evening. Thus, an evening carb-load may benefit from exercise to effectively partition the energy influx into skeletal muscle [and away from adipose tissue].
Summary of Part 1 of my CBL review: studies on nutrient timing sans exercise aren’t entirely consistent, in part, due to reciprocal regulation of insulin sensitivity in skeletal muscle and adipose tissue. That is, excess energy from an evening carb-load, without the exercise-induced, skeletal muscle-specific boost in insulin sensitivity, may be biased less toward muscle growth and more toward fat storage, because unlike skeletal muscle, the sensitivity of adipose tissue to insulin appears to improve as the day progresses… and without exercise to offset this, as in the studies discussed below, this may lead to suboptimal results.
*one thing Kiefer stressed, and I agree, is that the effects of any given intervention may be population-specific. For example, he pointed out that diurnal insulin sensitivity is less robust in obese and aged populations. So if two findings aren’t in full agreement, click the link to the study and check this first… context matters!
Carb Back-Loading, take II: More in-depth research to find the least fattening way to eat the wrong things. http://t.co/9RcEQrva4O
Tl;dr: I think high intensity exercise and possibly the time of day it’s performed, and regular bouts of fasting, are important factors that mediate the efficacy of CBL and similar protocols. Continue reading →
Step 1: eat little in the morning (maybe some fat+protein; definitely no carb)
Step 2: exercise in the afternoon/evening
Step 3: eat the carbs, all of them. Preferably high glycemic carbs.
Other: no dietary fat post-workout; protein periodically throughout the day.
What makes CBL different from its predecessors is the stress on the timing – exercise and carbs in the evening. John Berardi’s “Massive Eating” dietary guidelines are similar: protein+fat meals all day except pre- and post-workout, which are protein+carb meals. Martin Berkan’s “LeanGains” is fasting most of the time (including pre-workout), exercise in the afternoon, then a big post-workout meal (quite similar to CBL). My only tweak, as discussed below (and previously here and here), would be a pre- rather than post-workout meal [in some contexts].
There’s a summary of this blog post at the bottom… it might be helpful to read that first (see: “Tl;dr:”). Also, please note that much of this post is about the fringe of theoretically optimizing nutrient partitioning, like improving from 85 to 90%, or 40 to 45%, not 40 to 90%… I’m not that deluded.
My initial take, in general, is that this book is loaded with gems about nutrition, exercise, biochemistry, and physiology. It’s also very readable and has a lot of good recommendations. In this post, I want to discuss one specific aspect of CBL: tissue-specific circadian regulation of metabolism.
In this [pioneering] study, obese patients were subjected to a variety of performance assessments in a baseline period, then after 1 and 6 weeks of weight loss via protein-sparing modified fast (1.2 g/kg ideal body weight from lean meat, fish, or fowl; probably around 80 grams of protein/d, 500-750 kcal/d). They lost a lot of weight, 23 pounds on average, two-thirds of which was body fat. There was no exercise intervention, just the performance assessments.
During the ‘exercise to exhaustion’ treadmill exercise, RQ steadily declined from baseline to week 1 to week 6, indicating progressively more reliance on fat oxidation. This was confirmed via muscle glycogen levels pre- and post-exercise: during the baseline testing, they declined by 15%; after 6 weeks of ketoadaptation, however, they only declined by 2%, while ‘time to exhaustion’ increased by 55%. After only 1 week of the diet, time to exhaustion plummeted, as expected, by 20%.
This was, as mentioned above, a pioneering study in the field of ketoadaptation. It also challenges one of the prevailing theories of ‘fatigue’ …while carb-adapted, the subjects fatigued after 168 minutes, with muscle glycogen levels of 1.29 (reduced by 15%); while ketoadapted, they fatigued after 249 minutes with muscle glycogen levels of 1.02 (reduced by 2%). In other words, they had less glycogen to begin with, used less glycogen during exercise, and performed significantly better (running on fat & ketones).
Highly trained endurance athletes followed a high fat (53% fat, 32% carbs) or high carb (17% fat, 68% carbs) diet for 5 weeks in a randomized crossover study. In contrast to Phinney’s study, these participants were: 1) highly trained; and 2) exercised throughout the study.
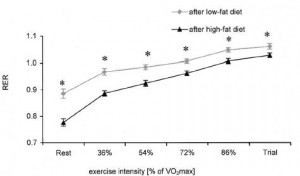
Maximal power output and VO2max during a similar ‘time to exhaustion’ test was similar after both diet periods. Same for total work output during a 20 minute ‘all-out’ cycling time trial and half-marathon running time. Muscle glycogen was modestly, albeit statistically non-significantly lower after ketoadaption; however, ketoadapted athletes relied on a higher proportion of fat oxidation to fuel performance as indicated by lower RQ at every level of exercise intensity:
Again, this is the essence of ketoadaptation. Physical performance as good as or better using fat and fat-derived fuels.
One reason Phinney’s glycogen-depeleted ketoadapted subjects may have done so well is their reliance on ketones (probable) and intramyocellular lipids (IMCL) (possible). In Vogt’s study, IMCL increased from 0.69 to 1.54% after ketoadaptation…
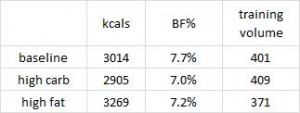
Also, food intake and body fat declined, and training volume increased in the low fat group; whereas food intake increased, and body fat and training volume declined in the high fat group. Reminiscent of anything?
High fat, low carb -> eat more, exercise less, STILL LOSE BODY FAT.
Sorcery? No. Diet impacts more than just mood and body composition – resting energy expenditure increased in the ketogenic dieters. This isn’t an isolated finding.
This was another study in non-trained athletes, consuming high fat (61% fat) or control (25% fat) diets for 6 weeks. The tests were the 30-second Wingate, to examine supramaximal performance, and a 45-minute timed ride, to examine submaximal performance.
This study differed from the previous two in several significant ways. For starters, peak power output declined in both groups, slightly more so in the high fat group (-10% vs. -8%). Furthermore, RQ didn’t wasn’t significantly lower during this test in the high fat group, which possibly suggests they weren’t properly ketoadapted. In Phinney’s study, the large energy deficit ensured ketoadaptation; this study lacked that aspect, somewhat more similar to Vogt’s, although unlike Vogt’s, these participants weren’t athletes which presumably makes ketoadaptation more difficult.
There are many factors at play… I wasn’t kidding when I said these studies are very nuanced!
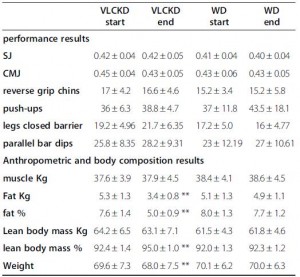
These were ‘elite artistic gymnasts,’ who could likely beat you in a race running backwards. The ketogenic phase consisted of 55% fat and much more protein than the control phase (39% fat; protein: 41% vs. 15%). The significantly higher protein content was modestly offset by slightly more calories in the control phase, which reduces the amount of protein required to maintain nitrogen balance.
In this study, performance was, for the most part, ‘maintained,’ with relative increases in a few of the tests; eg, the “legs closed barrier.” Changes in body composition were more robust: significantly reduced body fat and increased lean body mass after 30 days of ketogenic dieting (with their normal exercise routine).
The major confounder in this study was the use of an herbal cocktail only in the ketogenic diet group; despite this, the results are largely in line with the other studies. For more on this study, see here.
Exhibit E. the most dramatic one to date: Sawyer 2013
Please see here for the details, but in brief, strength-trained athletes showed improvements in high intensity exercise performance after only 7 days of carbohydrate restriction. The nuances of this particular study are discussed more here.
Collectively, these studies show that physical performance in both endurance and high intensity realms does not always suffer, can be maintained, and in some cases is improved by ketogenic dieting. Important factors are duration (to ensure adequate ketoadaptation), energy balance, and regular physical activity (athletes and regular exercisers can adapt to burning fat much quicker than sedentary folks).
Switch an athlete from their standard carbohydrate-rich diet to a low carb ketogenic one and suddenly performance tanks. It is known. Give them a few weeks to adapt, however, and it recovers. This much was established for mainly endurance-related performance parameters by Steve Phinney and colleagues in the 1980’s (eg, Phinney et al., 1983). Then, along came Antonio Paoli, Dominic D’Agostino, and others who showed a similar phenomenon in gymnasts, a population that routinely exercises at higher levels of intensity (Paoli et al., 2012). Notably, in these studies the athletes were allowed adequate time to adapt to the new metabolic milieu – sometimes referred to as ketoadaptation. Three weeks appears to be the minimum amount of time required for ketoadaptation; ie, studies of shorter duration generally show: low carb = poor physical performance.
These researchers subjected ~30 strength-trained individuals to a battery of performance assessments before and after 7 days of a low carb [ketogenic] diet. Usually I would’ve stopped reading at this point because 7 days is too short. But there were some nuances in the way this particular study was designed which piqued my interest.
Active individuals: 1.2-2.0 g/kg (via ISSN)
Comment (1): I think sedentary, physically inactive, and non-exercisers should be in this range to offset disuse atrophy. And they should exercise.
Comment (2): Do athletes really need more protein than non-athletes? They have exercise, a powerful anabolic stimulus. More protein may improve performance or body composition, but they might not *need* it, in terms of nitrogen retention… there’s probably a study on this.
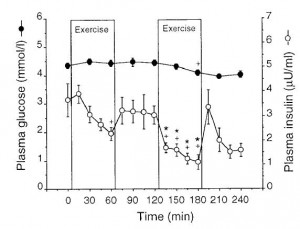
Insulin secretion is attenuated by sympathetic nervous system activity; eg, via exercise. Theoretically, exercising after a meal should blunt insulin secretion and I don’t think this will lessen the benefits of exercise, but rather enhance nutrient partitioning. And this isn’t about the [mythical?] post-workout “anabolic window.”
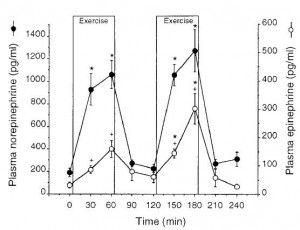
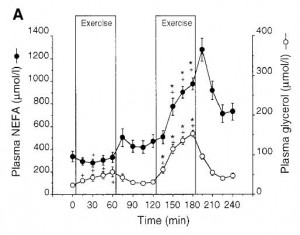
Sympathetic innervation of pancreas: norepinephrine –> adrenergic receptor activation = decreased insulin secretion & increased lipolysis (Stich et al., 1999):
note how quickly catecholamines are cleared upon exercise cessation