update: I learned a new trick. If you haven’t been receiving the regular updates to which you subscribed, it’s probably due to spam filters. Cure: find the update in your spam folder and reply to it. You don’t have to write anything, but the mere act of replying somehow tells your spam filter that the email wasn’t spam. It works for gmail, fwiw.
I [still] predict public approval of dietary fat will come along at a snail’s pace, and it won’t be a pan-approval of dietary fat at all. Instead, it will be selective approval of individual fatty acids. First, it was the medium chain fatty acids found in MCTs and coconut oil. Then, it was the fish oil fatty acids eicosapentaenoic and docosahexaenoic acids (EPA and DHA, respectively). Then, palmitoleic acid. Corn and soybean oil, on the other hand, are being appropriately recognized as bad. The utter hatred and fear of saturated fats is starting to wane, and we might even see a transition back to lard before I die (circa 2113). But today’s post is on another topic: trans fats, oxidized fish oils, and dairy fat.
As previously discussed, DRINK was a randomized intervention study that gave children either regular or diet soda for a year and surprise surprise, the regular soda drinkers gained about more body fat than the diet soda drinkers (de Ruyter et al., 2012). And in the follow-up, with an opposite study design, overweight & obese children who continued to drink regular soda gained twice as much weight as those who cut their intake (Ebbeling et al., 2012). There was no apparent black box in the latter study as the kids who stopped drinking soda also decreased their intake of other foods…
-does not compute-
wait a minute … By switching from regular soda to diet, you just end up compensating by eating more of something else, right? My initial response to that has always been that it doesn’t matter – ANYTHING else is better than a straight shot of 100% HFCS (+ some other chemicals). But those kids didn’t do that. they ate less of other foods.
Does HFCS soda make you eat more?
A recent study has put a little more fuel on this fire. Similar to the abovementioned two, it’s not a sophisticated study designed to accurately assess the impact of regular soda on appetite, satiety, hunger, etc., but it supports the theory that diet soda negative calories are NOT compensated for by eating more of something else.
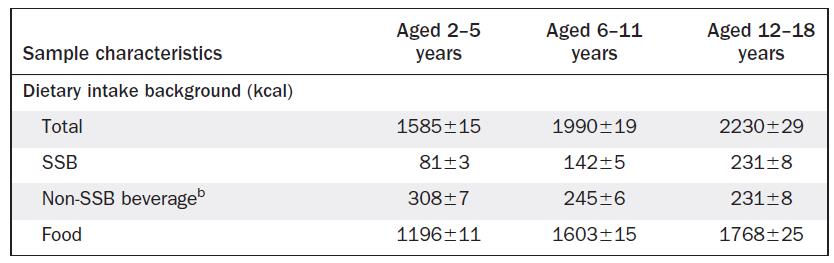
It was another big cross-sectional NHANES study that simply asked how much regular soda, diet soda, and other foods kids were eating.
They showed that as soda intake increased, so did total calories, which could simply mean the soda was adding calories to their diets. This would indirectly support the opposite of the above mentioned theory, namely, that soda calories aren’t compensated for. But it gets better (or worse, depending how you look at it):
soda didn’t simply add to the total calorie intake. More often than not, calorie intake increased above and beyond that contributed by the soda. And it wasn’t just that bigger kids were drinking more soda and eating more food – these data were controlled for body weight. The authors estimated that for every 100 kcal of soda drank, an additional 36 – 86 kcal of food was eaten.
salt makes you thirsty, and now soda makes you hungry?
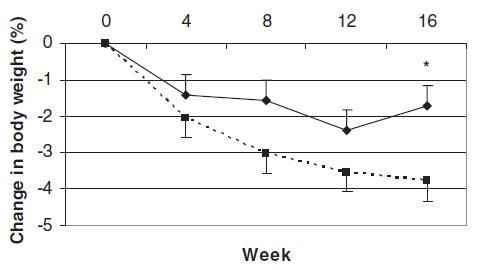
Take a group of obese people (> 250 lbs) and put them on a massive calorie restricted diet. They lose weight and metabolic rate plummets. Weight loss fail? In most cases, yes. But a recent study showed that the decrepit post-weight loss metabolic rate gradually improves in parallel with an increase in dietary fat ingestion to such a degree that even after two long years: totally food intake was almost back to normal, energy expenditure improved, and all this happened despite continual weight loss. In other words, obesity is not permanent.
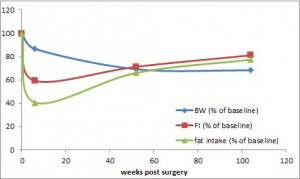
Statistically speaking, no diet on Earth comes close to RYGB in terms of weight loss success. Long term. Seemingly permanent. It’s the closest thing to a cure we’ve got.
Body weight is down by 30%, and energy expenditure is rising faster than a speeding bullet. because food intake is increasing while body weight is dropping – they’re probably more active too ** weight loss than more exercise –
But there’s a more mystical aspect to RYGB that warrants attention. (it could be the increasing fat intake, but for now let’s just say it’s RYGB per se). According to this pearl, weight loss of only 10% via diet alone causes energy expenditure crash by 394-500 kcal/d, and physiological replacement of leptin via subcutaneous injection can increase this by 234-454 kcal/d (Rosenbaum, Murphy, Heymsfield, Matthews, and Leibel, 2002).
It is speculated: niacin binds a particular “ketone” receptor (GPR109?) (physiological relevance?).
It is known: niacin is ketogenic in rats. Repeat: niacin is ketogenic in rats.
Niacin aka nicotinic acid and nicotamide aka niacinamide both fulfill the requirement for Vitamin B3 (ie, prevent pellagra). But only the former causes flushing… and only the former is ketogenic (two apparently unrelated phenomena).
Whether you’re strictly adhering to a diet or just doing your own thing, if year after year your GP is prescribing more and more medications to stave off morbidity and keep you intact, then the diet you’re following is most likely Fail. The same is true if your body weight is creeping upward or your quality of life is creeping downward.
The glaring Fail of all 3 diets in the recent Mediterranean Diet Study for the medications criteria threw up a huge red flag. As a brief refresher, at baseline and 5 years later, prescription medication usage was as follows:
Part I. Ketones are made from fat in the liver. But dietary fat has a lot of places to go and people to see, so it rarely gets to the liver en masse to a degree great enough to stimulate ketosis. Not so much for medium chain triglycerides (MCTs). Upon entry (ingestion), MCTs go to the liver and are metabolized to ketones without passing GO or collecting $200… but is this sufficient to reap the benefits of a ketogenic diet?
MCTs (C8-10) comprise ~14 of the fat in coconut oil, and 9.2% in dairy. As such, average MCT intake is low – ~2% of total fat intake [because we eat a lot of vegetable oil and not a lot of coconuts].
Healthy people assigned to either ~21grams of either MCTs or olive oil (~12% of total calories on a hypocaloric 1650 kcal/d weight loss diet) for 16 weeks:
This is one of the biggest diet studies we’ve seen in a while, and no doubt it was a very good one. It very effectively put the Mediterranean Diet to the test.
I felt compelled to write about this study out of fear for the nutrition disinformation that it would likely inspire. The Mediterranean Diet is associated with all good things, happiness, red wine and olive oil; whereas the Atkins Diet is associated with artery clogging bacon-wrapped hot dogs and a fat guy who died of a heart attack. Nutrition disinformation.
If you ran a diet study with 3 intervention groups for 5 years, and by the end of the study everybody (in all 3 groups) was on more prescription medications, would you conclude any of the diets were “healthy?” If so, then we should work on your definition of “healthy.”
Study details: big study, lasted roughly 5 years, and the diet intervention was pristine. Mediterranean diet plus extra virgin olive oil (EVOO) vs. Mediterranean diet plus nuts vs. low fat control. They even used biomarkers to confirm olive oil and nut intake (hydroxytyrosol and linoleate, respectively). Compliance was good.
While it has a decent amino acid profile, with only 3 grams of protein it’d take a diabetic amount of potatoes to fulfill your daily protein. By “diabetic,” I mean about a thousand grams of starch. potatoes are just as glycemic as white bread.
No, not heavyweight powerhouses. Mitochondria IN fat cells. electricity is required for your space heater, not your long johns.
At first glance, the mere presence of mitochondria in adipocytes seems perplexing. On one hand, there’s tons of fat to burn, so why not have the capacity to do it? Well yeah, but on the other hand, adipose doesn’t do very much. It doesn’t contract like skeletal muscle or crank out glucose like liver. Mitochondria in BAT is understandable, to generate heat and what not. electricity is required for your space heater, not your long johns.
My best guess is that adipose tissue mitochondria are there to do something else – make shorter acyl chained FA’s, or free radicals, etc., to signal something. Just not primarily to generate energy.
But drop an anvil on adipose tissue mitochondria and you get some interesting mice indeed. Impossible mice.
TFAM – in brief, the enzyme that goes by the acronym TFAM makes mitochondria work. Global TFAM KO is lethal. But adipose tissue (AT)-specific KO is interesting. Uncoupling goes through the roof and fat literally burns away. kind of***.
As much as I’d like to say this is the nail-in-the-coffin, omega-6 causes irreversible fatality, I have a confession.
I believe it’s the empty calories, not the inflammatory omega-6 devil linoleate. Biscuits, cookies, processed foods of all shapes and sizes are simply the delivery vehicles for industrially modified and probably “trans” fats that started out innocent enough as soybean oil or omega-6 vegetable oils.
linoleate is the quintessential omega-6 fatty acid and is found at high levels in vegetable oils. just like the omega-3 linolenate found in soybean oil, processing of the oils usually damages them – turns them into trans fats and/or oxidizes them (by “oxidizes” I don’t mean fat burning, see pictorial below)
So despite the impeccable statistical anvil thrown at these data, which seem to clearly implicate linoleate, I don’t think it’s the linoleate. H E double hockey sticks, we probably don’t get enough normal unmodified linoleate. Unless you’re cracking shells, even “raw” almonds are Pasteurized.
don’t sanitize your food. your meat needn’t be burned, nor your nuts Pasteurized.