Marijuana is a very complex plant: many different strains with differing profiles of psychoactive, non-psychoactive, and peripherally-active compounds that impact metabolism. Most have THC, which activates endogenous cannabinoid receptors and mimics many of the effects of smoked marijuana (eg, see studies by Hart, Wachtel, and Curran).
Do not underestimate the complexity of this plant.

“LOL”
I’m not ‘anti-pot’ as there are far worse drugs out there… however, some advocates make really bad “pro” arguments, like saying it’s actually healthy (or at least not harmful in any way)…
there are many independent lines of evidence which suggest otherwise, metabolically speaking.
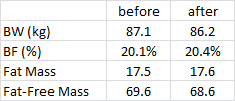
Rimonabant, the notorious pot-blocker, reduces appetite and is a fairly effective weight loss drug, but has the unfortunate side effect of doing the opposite of marijuana, psychologically speaking. See any of the RIO studies, eg:
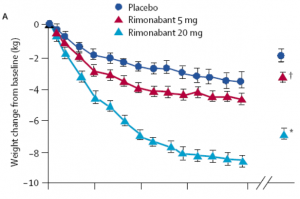
All participants lost weight and experienced improved metabolic profiles, insulin sensitivity, etc., by blocking endogenous cannabinoid receptors.
Adverse effects? Wellll, there’s a drug called Marinol (pure THC) that’s technically an anti-emetic (reduces the urge to vomit); it improves appetite in patients with conditions associated with anorexia or wasting. It’s a cannabinoid agonist. Blocking CB1 with Rimonabant induces nausea in some patients: no bueno, but not unexpected given the known effects of Marinol. Rimonabant is also associated with depression and anxiety (in some patients); also not unexpected.
So, it’s not a good idea to block this receptor pharmacologically (for psychological reasons) or activate it recreationally (for metabolic reasons). Obesity researchers (and big pharma no doubt) are still looking for a pot-blocker that doesn’t penetrate the brain to avoid the negative psychological side effects (eg, Klumpers et al., 2013).
Best. Graph. Ever. The effect of Rimonabant on how stoned participants felt after smoking pot. Yes, “Stoned” was published in the Journal of the American Medical Association (Huestis et al., 2001).

Indeed, Rimonabant effectively treats “cannabis intoxication” (Crippa et al., 2012). Antagonist versus agonist 101.
Part II: the biological effects of cannabis, THC, marijuana, and antagonists, etc.
THC acts like insulin on adipocytes: increased adipogenesis, fatty acid uptake, and decreased lipolysis (eg, see studies by Teixeira and Cota). Munchies, anyone?
Cannabinoids and mimetics/agonists induce hunger and repress satiety; cannabinoid blockers induce satiety and weight loss. However, I actually don’t think marijuana is obesogenic aside from its anti-anorexic effects. Cannabis use is not always associated with obesity, possibly due to confounding and/or the lack of good crossover studies (you can’t really do a proper study in healthy humans with MJ for ethical reasons). But most rodent studies agree that cannabinoids, acting via cannabinoid receptors, induce metabolic syndrome-like effects in nearly every single tissue and on the whole-body level.
CB1 cannabinoid receptor deletion in mice leads to leanness, resistance to diet-induced obesity, and enhanced leptin sensitivity (Trillou et al., 2003). For context, mice lacking CB1 is somewhat analogous to humans not smoking marijuana.
In liver, cannabinoid signaling induces fat accumulation and insulin resistance (Osei-Hyiaman et al., 2008). This is absent in CB1 and liver-specific CB1 knockout models. Mice overexpressing this receptor in liver exhibit increased insulin resistance (Liu et al., 2012).
Activating cannabinoid receptor-2 (CB2) causes insulin resistance and adipose tissue inflammation, and this is blunted in mice lacking CB2 (Deveaux et al., 2009).
The knockouts & over-expressing rodent models, and pharmacological agonist & antagonist studies are all consistent. That said, I still don’t think this is the worst recreational drug out there, even among “legal” ones.
Check out my Patreon campaign! Full access for a five bucks a month and there are many other options. It’s ad-free and you can cancel if it sucks 🙂
If you’re interested in personalized health consulting services, send me an email:drlagakos@gmail.com.
Affiliate links: KetoLogic for keto-friendly shakes, creamers, snacks, etc. And get 15% off your ketone measuring supplies HERE.
Still looking for a pair of hot blue blockers? TrueDark is offering 10% off HERE and Spectra479 is offering 15% off HERE. If you have no idea what I’m talking about, read this then this.
Join Binance and get some cryptoassets or download Honeyminer and get some Bitcoins for free!
20% off some delish stocks and broths from Kettle and Fire HERE.
If you want the benefits of ‘shrooms but don’t like eating them, Real Mushrooms makes great extracts. 10% off with coupon code LAGAKOS. I recommend Lion’s Mane for the brain and Reishi for everything else.
Join Earn.com with this link.
Start your OWN Patreon campaign!
calories proper