The regulation of energy balance is a long-term process, and it can’t be maintained by counting calories on a day-to-day basis. Taubes once wrote that exercise doesn’t cause weight loss because it builds up an appetite, so you end up sucking down a Starbuck’s Jumbo Calorie Bomb on the way home from doing Yoga at the gym. This is probably somewhat true, but this little gem from 1955 exposes some very interesting nuances.
These researchers rigorously measured food intake and did a comprehensive assessment of energy expenditure during a wide variety of activities – lying down, standing, walking, gun cleaning, stair climbing, dressing, etc., etc.
Divide and conquer
The individual differences: big people expend more energy on life. most of the time.
The day you’ve all been waiting for has finally arrived. Results from the Look AHEAD study have been published. When I first wrote about this study (HERE), it had been prematurely halted because the intervention was providing no benefits. Everybody was in a state of shock and awe because Low Fat didn’t save lives. But that was before we even had the data.
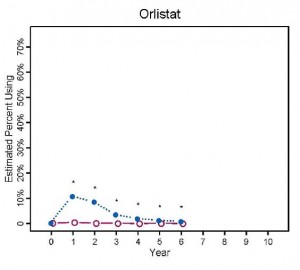
Reminder: the “intensive lifestyle intervention” consisted of a Low Fat Diet & exercise. The results? Yes, they lost more weight than control, but they also took more Orlistat (of which I’m not a fan, see HERE for why):
Their normal diets were not healthy, but neither was low fat –>
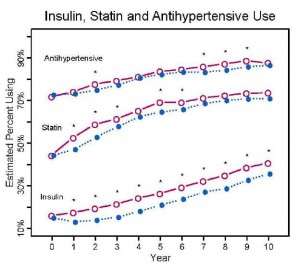
Medication use increased drastically in both groups. The pundits have gone wild because medication use was lower in the intensive Low Fat group at the end of the study, but this is Nutrition Disinformation 2.0. Eerily reminiscent of the recent Mediterranean Diet study, the conclusions are the same: keep eating poorly and the need for medications will increase. You can call it a lot of things, but not “healthy.” The alternative –> How to define a “healthy” diet. Period.
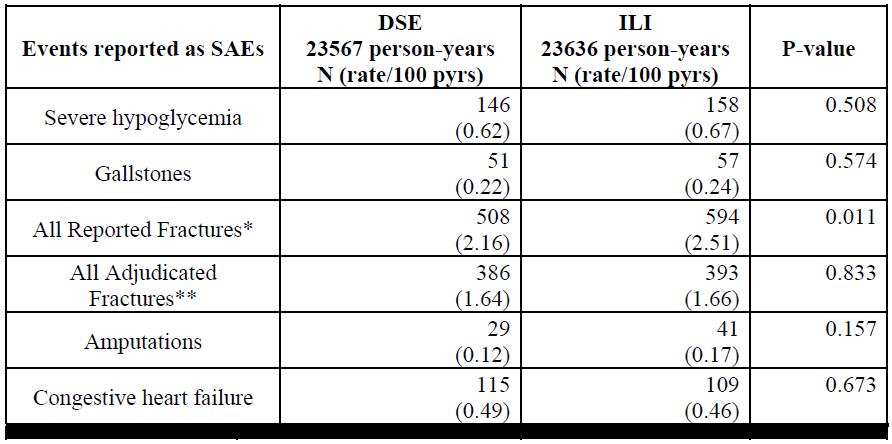
Significant adverse events:
The only thing to reach statistical significance was more fractures in the intensive Low Fat group, but you didn’t read any headlines that said “Low Fat breaks bones.” Imagine if that happened on low carb [sigh] The next closest thing to statistical significance was increased amputations in the intensive Low Fat group :/
gem:
Translation: if you were healthy at baseline, then you could tolerate a low fat diet. Otherwise, not so much. This is exactly what happened in the Women’s Health Initiative.
needless to say, none of the “possible explanations” they considered were Low fat diet Fail.
Lots of metabolism talk below, but first a brief intro. My “muse,” if you will.
Taubes’ recent article in the BMJ (Taubes, 2013; full text) generated some interesting feedback.
In the original article, Taubes basically re-states his philosophy on obesity. Nothing new. But one rebuttal by Cottrell got under my skin (Cottrell, 2013), and Taubes’ response was woefully inadequate.
Cottrell [sic]: “A third incorrect assertion is that obesity can be attributed to the conversion of carbohydrate to fat. This is an unsatisfactory explanation of obesity, because this route is a minor pathway to depot fat in humans, even under conditions of substantial overfeeding of sugars to obese subjects. An unproved assumption is that the hypothetical diversion of carbohydrate energy into fat storage leaves the subject hungry, thus stimulating overeating.”
Cottrell set up a straw man and handily took it down. The primary mechanism whereby excess carbs contribute to obesity is via insulin’s effects on adipose tissue. Even if you’re eating very little fat, insulin will cause it to get stored. Insulin is very good at this – it is actually far more potent at stimulating fat storage than it is at stimulating glucose uptake (eg, Insulin vs. fat metabolism FTW). Cottrell’s straw man is that excess carbs themselves are stored as fat. This does not occur to any appreciable extent in humans. Here is why I believe that to be true, from one of most insightful and informative studies on the topic IMHO.
MCTs provide a respectable boost in diet-induced thermogenesis (in some studies [eg, Kasai 2002 & Clegg 2012], but not others [Alexandrou 2007]), but I don’t think that’s what does it.
The alternative? MCTs aren’t “linoleate.” (sorry for lack of suspense)
Further, feed rats a diet rich in either coconut oil, olive oil, safflower oil, evening primrose oil, or menhaden oil… and eventually the fat stored in their bodies reflect those fats – eg, linoleate only accumulated in the tissues of those fed safflower & evening primrose oils (Yaqoob 1995) (expect similar results with soybean & corn oils).
Researchers constantly refer to MCTs & coconut oil as “saturated fats,” but I always thought the chain length should be recognized. Perhaps. But with regard to certain benefits (eg, hepatoprotection), perhaps not.
Cacao butter has a lot of stearate (a fully saturated 18-carbon fatty acid) but not much linoleate or MCTs. This linoleate may very well be more of a detriment than stearate or MCTs are a benefit… (with regard to certain benefits [eg, hepatoprotection])
Once thought to be the holy grail of energy expenditure manipulators and a potential cure for obesity – fail. I don’t have great evidence for this; it’s really just a hunch.
A new mouse study has provided some additional fodder for speculation, however.
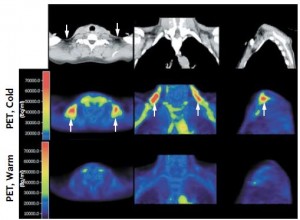
In a slurry of publications in 2009, researchers re-ignited the quest by showing cold-induced BAT activation in healthy humans (Virtanen et al., 2009):
Proceed with caution, this is an exploratory post. Replacing CakesCookiesPiesPastriesBreadCerealsBiscuitsPizzaMuffins with [insert any whole food item here] is just a good idea. And more reasons to eat dark chocolate.
In Inflammatory, trans, or linoleate? the idea was explored that it might not be the theorized textbook pro-inflammatory end products of omega-6 fats that give them a bad rap, but rather the foods that contain them – ie, “cakes, cookies, pies, and pastries” (Kris-Etherton et al., 2012 NHANES), or “bread, cereals, cakes, biscuits, pies, pizza, and muffins” (Meyer et al., 2003 from down under).
Further, what starts out as an omega-6 fat can easily become peroxidized or isomerized into an oxidized or trans fat, respectively, via industrial molestation or just plain old cooking (eg, Romero et al., 1998, Marmesat et al., 2012, & Minami et al., 2012) – even just a few minutes in the microwave (Herzallah et al., 2005)! I don’t know exactly what all of these end products are for sure, but they might look something like this:
Thus, the culprit may not be native Dc9,c1218:2n6 linoleate.
What to serve with a liquid lunch, and a recipe for chocolate.
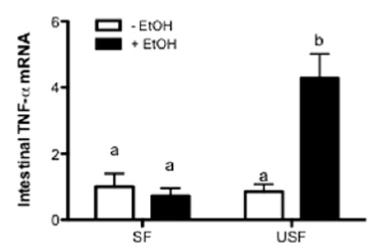
It’s like a feed forward downward spiral. If you don’t eat saturated fat & MCTs prior to imbibing, then liver intentionally makes more PUFAs for the alcohol-induced burning ROS to molest. Liver is evil but need not be punished. SFAs.
Researchers studying alcohol in rodents know where they’re going and like to get there fast. 70 drinks per day fast. Granted, rats metabolize faster than humans so it’s likely a little less… but a little less than 70 is still a lot of sauce.
update: I learned a new trick. If you haven’t been receiving the regular updates to which you subscribed, it’s probably due to spam filters. Cure: find the update in your spam folder and reply to it. You don’t have to write anything, but the mere act of replying somehow tells your spam filter that the email wasn’t spam. It works for gmail, fwiw.
I [still] predict public approval of dietary fat will come along at a snail’s pace, and it won’t be a pan-approval of dietary fat at all. Instead, it will be selective approval of individual fatty acids. First, it was the medium chain fatty acids found in MCTs and coconut oil. Then, it was the fish oil fatty acids eicosapentaenoic and docosahexaenoic acids (EPA and DHA, respectively). Then, palmitoleic acid. Corn and soybean oil, on the other hand, are being appropriately recognized as bad. The utter hatred and fear of saturated fats is starting to wane, and we might even see a transition back to lard before I die (circa 2113). But today’s post is on another topic: trans fats, oxidized fish oils, and dairy fat.
As previously discussed, DRINK was a randomized intervention study that gave children either regular or diet soda for a year and surprise surprise, the regular soda drinkers gained about more body fat than the diet soda drinkers (de Ruyter et al., 2012). And in the follow-up, with an opposite study design, overweight & obese children who continued to drink regular soda gained twice as much weight as those who cut their intake (Ebbeling et al., 2012). There was no apparent black box in the latter study as the kids who stopped drinking soda also decreased their intake of other foods…
-does not compute-
wait a minute … By switching from regular soda to diet, you just end up compensating by eating more of something else, right? My initial response to that has always been that it doesn’t matter – ANYTHING else is better than a straight shot of 100% HFCS (+ some other chemicals). But those kids didn’t do that. they ate less of other foods.
Does HFCS soda make you eat more?
A recent study has put a little more fuel on this fire. Similar to the abovementioned two, it’s not a sophisticated study designed to accurately assess the impact of regular soda on appetite, satiety, hunger, etc., but it supports the theory that diet soda negative calories are NOT compensated for by eating more of something else.
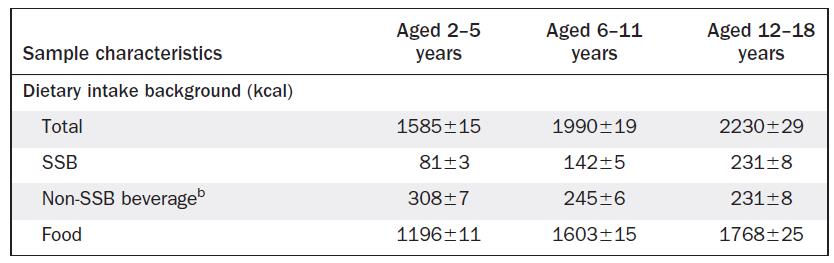
It was another big cross-sectional NHANES study that simply asked how much regular soda, diet soda, and other foods kids were eating.
They showed that as soda intake increased, so did total calories, which could simply mean the soda was adding calories to their diets. This would indirectly support the opposite of the above mentioned theory, namely, that soda calories aren’t compensated for. But it gets better (or worse, depending how you look at it):
soda didn’t simply add to the total calorie intake. More often than not, calorie intake increased above and beyond that contributed by the soda. And it wasn’t just that bigger kids were drinking more soda and eating more food – these data were controlled for body weight. The authors estimated that for every 100 kcal of soda drank, an additional 36 – 86 kcal of food was eaten.
salt makes you thirsty, and now soda makes you hungry?
Take a group of obese people (> 250 lbs) and put them on a massive calorie restricted diet. They lose weight and metabolic rate plummets. Weight loss fail? In most cases, yes. But a recent study showed that the decrepit post-weight loss metabolic rate gradually improves in parallel with an increase in dietary fat ingestion to such a degree that even after two long years: totally food intake was almost back to normal, energy expenditure improved, and all this happened despite continual weight loss. In other words, obesity is not permanent.
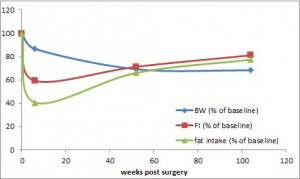
Statistically speaking, no diet on Earth comes close to RYGB in terms of weight loss success. Long term. Seemingly permanent. It’s the closest thing to a cure we’ve got.
Body weight is down by 30%, and energy expenditure is rising faster than a speeding bullet. because food intake is increasing while body weight is dropping – they’re probably more active too ** weight loss than more exercise –
But there’s a more mystical aspect to RYGB that warrants attention. (it could be the increasing fat intake, but for now let’s just say it’s RYGB per se). According to this pearl, weight loss of only 10% via diet alone causes energy expenditure crash by 394-500 kcal/d, and physiological replacement of leptin via subcutaneous injection can increase this by 234-454 kcal/d (Rosenbaum, Murphy, Heymsfield, Matthews, and Leibel, 2002).