Hat tip to Jane Plain and her ongoing series on “The physiology of body fat regulation” for citing this study as it provides a rather interesting insight into the psychoendoneuropathophysiology of the obese condition. Eating in the Absence of Hunger.
They were all full or half, weight-discordant, same-sex siblings and each sibling pair had the same mother; same mitochondrial DNA, shared a womb, etc.
MCTs provide a respectable boost in diet-induced thermogenesis (in some studies [eg, Kasai 2002 & Clegg 2012], but not others [Alexandrou 2007]), but I don’t think that’s what does it.
The alternative? MCTs aren’t “linoleate.” (sorry for lack of suspense)
Further, feed rats a diet rich in either coconut oil, olive oil, safflower oil, evening primrose oil, or menhaden oil… and eventually the fat stored in their bodies reflect those fats – eg, linoleate only accumulated in the tissues of those fed safflower & evening primrose oils (Yaqoob 1995) (expect similar results with soybean & corn oils).
Researchers constantly refer to MCTs & coconut oil as “saturated fats,” but I always thought the chain length should be recognized. Perhaps. But with regard to certain benefits (eg, hepatoprotection), perhaps not.
Cacao butter has a lot of stearate (a fully saturated 18-carbon fatty acid) but not much linoleate or MCTs. This linoleate may very well be more of a detriment than stearate or MCTs are a benefit… (with regard to certain benefits [eg, hepatoprotection])
Once thought to be the holy grail of energy expenditure manipulators and a potential cure for obesity – fail. I don’t have great evidence for this; it’s really just a hunch.
A new mouse study has provided some additional fodder for speculation, however.
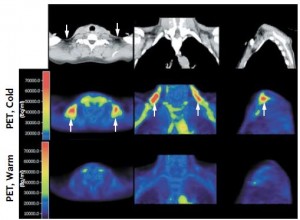
In a slurry of publications in 2009, researchers re-ignited the quest by showing cold-induced BAT activation in healthy humans (Virtanen et al., 2009):
Proceed with caution, this is an exploratory post. Replacing CakesCookiesPiesPastriesBreadCerealsBiscuitsPizzaMuffins with [insert any whole food item here] is just a good idea. And more reasons to eat dark chocolate.
In Inflammatory, trans, or linoleate? the idea was explored that it might not be the theorized textbook pro-inflammatory end products of omega-6 fats that give them a bad rap, but rather the foods that contain them – ie, “cakes, cookies, pies, and pastries” (Kris-Etherton et al., 2012 NHANES), or “bread, cereals, cakes, biscuits, pies, pizza, and muffins” (Meyer et al., 2003 from down under).
Further, what starts out as an omega-6 fat can easily become peroxidized or isomerized into an oxidized or trans fat, respectively, via industrial molestation or just plain old cooking (eg, Romero et al., 1998, Marmesat et al., 2012, & Minami et al., 2012) – even just a few minutes in the microwave (Herzallah et al., 2005)! I don’t know exactly what all of these end products are for sure, but they might look something like this:
Thus, the culprit may not be native Dc9,c1218:2n6 linoleate.
What to serve with a liquid lunch, and a recipe for chocolate.
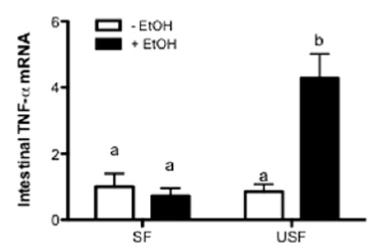
It’s like a feed forward downward spiral. If you don’t eat saturated fat & MCTs prior to imbibing, then liver intentionally makes more PUFAs for the alcohol-induced burning ROS to molest. Liver is evil but need not be punished. SFAs.
Researchers studying alcohol in rodents know where they’re going and like to get there fast. 70 drinks per day fast. Granted, rats metabolize faster than humans so it’s likely a little less… but a little less than 70 is still a lot of sauce.
update: I learned a new trick. If you haven’t been receiving the regular updates to which you subscribed, it’s probably due to spam filters. Cure: find the update in your spam folder and reply to it. You don’t have to write anything, but the mere act of replying somehow tells your spam filter that the email wasn’t spam. It works for gmail, fwiw.
I [still] predict public approval of dietary fat will come along at a snail’s pace, and it won’t be a pan-approval of dietary fat at all. Instead, it will be selective approval of individual fatty acids. First, it was the medium chain fatty acids found in MCTs and coconut oil. Then, it was the fish oil fatty acids eicosapentaenoic and docosahexaenoic acids (EPA and DHA, respectively). Then, palmitoleic acid. Corn and soybean oil, on the other hand, are being appropriately recognized as bad. The utter hatred and fear of saturated fats is starting to wane, and we might even see a transition back to lard before I die (circa 2113). But today’s post is on another topic: trans fats, oxidized fish oils, and dairy fat.
As previously discussed, DRINK was a randomized intervention study that gave children either regular or diet soda for a year and surprise surprise, the regular soda drinkers gained about more body fat than the diet soda drinkers (de Ruyter et al., 2012). And in the follow-up, with an opposite study design, overweight & obese children who continued to drink regular soda gained twice as much weight as those who cut their intake (Ebbeling et al., 2012). There was no apparent black box in the latter study as the kids who stopped drinking soda also decreased their intake of other foods…
-does not compute-
wait a minute … By switching from regular soda to diet, you just end up compensating by eating more of something else, right? My initial response to that has always been that it doesn’t matter – ANYTHING else is better than a straight shot of 100% HFCS (+ some other chemicals). But those kids didn’t do that. they ate less of other foods.
Does HFCS soda make you eat more?
A recent study has put a little more fuel on this fire. Similar to the abovementioned two, it’s not a sophisticated study designed to accurately assess the impact of regular soda on appetite, satiety, hunger, etc., but it supports the theory that diet soda negative calories are NOT compensated for by eating more of something else.
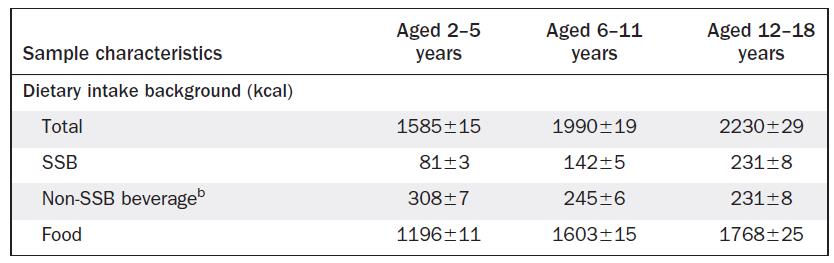
It was another big cross-sectional NHANES study that simply asked how much regular soda, diet soda, and other foods kids were eating.
They showed that as soda intake increased, so did total calories, which could simply mean the soda was adding calories to their diets. This would indirectly support the opposite of the above mentioned theory, namely, that soda calories aren’t compensated for. But it gets better (or worse, depending how you look at it):
soda didn’t simply add to the total calorie intake. More often than not, calorie intake increased above and beyond that contributed by the soda. And it wasn’t just that bigger kids were drinking more soda and eating more food – these data were controlled for body weight. The authors estimated that for every 100 kcal of soda drank, an additional 36 – 86 kcal of food was eaten.
salt makes you thirsty, and now soda makes you hungry?
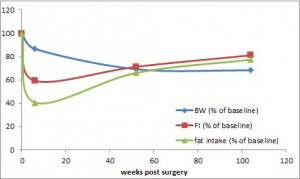
Take a group of obese people (> 250 lbs) and put them on a massive calorie restricted diet. They lose weight and metabolic rate plummets. Weight loss fail? In most cases, yes. But a recent study showed that the decrepit post-weight loss metabolic rate gradually improves in parallel with an increase in dietary fat ingestion to such a degree that even after two long years: totally food intake was almost back to normal, energy expenditure improved, and all this happened despite continual weight loss. In other words, obesity is not permanent.
Statistically speaking, no diet on Earth comes close to RYGB in terms of weight loss success. Long term. Seemingly permanent. It’s the closest thing to a cure we’ve got.
Body weight is down by 30%, and energy expenditure is rising faster than a speeding bullet. because food intake is increasing while body weight is dropping – they’re probably more active too ** weight loss than more exercise –
But there’s a more mystical aspect to RYGB that warrants attention. (it could be the increasing fat intake, but for now let’s just say it’s RYGB per se). According to this pearl, weight loss of only 10% via diet alone causes energy expenditure crash by 394-500 kcal/d, and physiological replacement of leptin via subcutaneous injection can increase this by 234-454 kcal/d (Rosenbaum, Murphy, Heymsfield, Matthews, and Leibel, 2002).
Whether you’re strictly adhering to a diet or just doing your own thing, if year after year your GP is prescribing more and more medications to stave off morbidity and keep you intact, then the diet you’re following is most likely Fail. The same is true if your body weight is creeping upward or your quality of life is creeping downward.
The glaring Fail of all 3 diets in the recent Mediterranean Diet Study for the medications criteria threw up a huge red flag. As a brief refresher, at baseline and 5 years later, prescription medication usage was as follows:
This is one of the biggest diet studies we’ve seen in a while, and no doubt it was a very good one. It very effectively put the Mediterranean Diet to the test.
I felt compelled to write about this study out of fear for the nutrition disinformation that it would likely inspire. The Mediterranean Diet is associated with all good things, happiness, red wine and olive oil; whereas the Atkins Diet is associated with artery clogging bacon-wrapped hot dogs and a fat guy who died of a heart attack. Nutrition disinformation.
If you ran a diet study with 3 intervention groups for 5 years, and by the end of the study everybody (in all 3 groups) was on more prescription medications, would you conclude any of the diets were “healthy?” If so, then we should work on your definition of “healthy.”
Study details: big study, lasted roughly 5 years, and the diet intervention was pristine. Mediterranean diet plus extra virgin olive oil (EVOO) vs. Mediterranean diet plus nuts vs. low fat control. They even used biomarkers to confirm olive oil and nut intake (hydroxytyrosol and linoleate, respectively). Compliance was good.