
Regular followers of this blog (all 3 of you) know I think positively about carbohydrate-restricted diets. In randomized controlled intervention studies, low-carb diets are a little better most of the time compared to low calorie and low fat diets (note the italics). They are healthier and there is probably no end to the benefits of chronically lower insulin levels. The only relevant disadvantage is that [I thought] such a diet requires too big of a change for most peoples lifestyle… however, this might not be the case. In light of some recent [relatively unscientific] findings, that change might not be so big after all.
In one study, Feinman and colleagues (Feinman et al., 2006 Nutrition Journal) surveyed a group of low carb dieters from the “Active Low-Carber Forum” about their diets. There was no formal subject recruitment or randomization; it was just a bunch of people who were following various low carb diets. The only requirement was that they were actually following a low carb diet for weight loss. For starters, there were a LOT of people who lost a LOT of weight: 62% of ~86,000 participants lost at least 30 pounds and kept it off for over a year (I know I know, it’s possible that people who lose a lot of weight are selectively more likely to participate on this particular forum [this study is confounded out the wazoo but still had a few pearls]).
What I found most interesting was what these people said were their biggest dietary changes. The top 2 were, not surprisingly, avoiding sugar and starch. Number 3 was drinking more water. So to sum up the top 3 changes: basic healthy dieting 101; not drastic lifestyle alterations.
Number 4 was the biggie: most people increased their green vegetable intake by over half… not bacon, hot dogs, and red meat… leafy greens. This is great (just think of all those micronutrients). They weren’t counting calories or replacing everything in their refrigerator; they were avoiding sugar and eating more leafy greens.

leafy greens: winner
sounds easy, right? Of course eating more protein and fat also occurred, but it wasn’t a universal requirement: only 5% reported increasing beef, butter, and bacon… instead, people just ate a little more of whatever was most convenient for their lifestyle.
This study changed my view. These people lost over 30 pounds on low carb and kept it off for over a year without making any huge changes.
Another more recent study (Kirk et al., 2012 Journal of Pediatrics) was a diet intervention study in obese children. They compared a low carb diet (LC), low glycemic index diet (RGL), and a portion controlled diet (PC).
It’s hard to put kids on a low carb diet. Indeed, adherence to the low carb diet was horrific, less than 30% at 3 months and down to 20% at 6 months (figure below on the right). But comparing this to the figure on the left is astonishing. Despite adherence of only around 25%, low carb dieters had the biggest reduction in body fat. It’s not until adherence was nil that the kids starting gaining weight back.
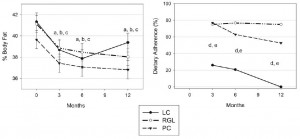
weight loss vs. adherence
What does this say about low carb? it’s the easiest diet in the world, even if you can barely follow it! 25% adherence to a low carb diet resulted in greater fat loss than 80% adherence to the other diets.
You might just be better off half-assing a low carb diet than strictly adhering to any another one-































