Potential conclusion (pending full texts): “if you’re gonna keto, no need to carb”
I think these three abstracts are all referring to the same studies. I haven’t seen the full texts. My takes are in italics, after each abstract.
Exhibit A. The Effects of an Eight Week Ketogenic Diet vs. a Cyclical Ketogenic Diet on Performance and Testosterone in a Resistance Training Program (Lane, Lowery, Volek, D’Agostino, Wilson, et al., 2015)
Introduction: Our lab recently examined the effects of the ketogenic diet (KD) compared to a western diet regarding strength related performance; additionally, free and total testosterone was evaluated. Individuals on the KD saw similar adaptations in strength and similar changes testosterone. Comparisons of the KD against a cyclic (CKD) in strength, endurance, and testosterone have not been previously demonstrated in literature.
Purpose: Therefore the purpose of this study was to investigate the effects of the KD versus a CKD on performance and testosterone in resistance-trained males.
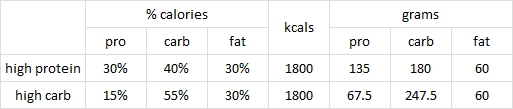
Methods: Sixteen resistance trained males participated in the study (age: 23.5 ± 3.3; weight: 187.6 ± 32.6). Participants on the KD consumed 5% carbohydrate, 25% protein, and 70% fat for 8 weeks. The CKD group applied the same macronutrient ratio to their diet Monday through Friday, while altering the ratio on weekends (50% carbohydrate, 25% protein, 25% fat). A periodized resistance training program was strictly followed 3 days per week throughout the duration of the study with high intensity interval training implemented on intermittent days 2 times per week by all participants. Participants were placed on a 500 kcal deficit derived from basal metabolic rate determined by the Mifflin St. Jeor equation. One repetition maximum (1RM) strength was assessed on deadlift, bench press, and leg press at baseline with a repeat assessment performed Week 8. Strength endurance was assessed on the leg press at baseline and re-assessed at Week 8. Free and total testosterone was evaluated at baseline and at Week 8. An ANOVA with repeated-measures was used to scrutinize the effects of KD and CKD on dependent variables assuming group (KD and CKD) and time (pre and post) as fixed factors. The significance level was set at p ? 0.05.
Results: There were no differences between groups in the performance tests or testosterone levels detected at baseline (p > 0.05). A time effect was observed for bench press and deadlift 1RM (p < 0.01). There was a trend towards a group by time interaction (p = 0.07) which favored an increase in the leg press 1RM in the KD group. There were no significant differences for leg press strength endurance in both groups. For free testosterone, there were no group or group × time interactions (p > 0.05). For total testosterone, there was a group × time interaction following the diet treatment (p < 0.02). The pairwise comparisons revealed that only the cyclic group decreased in total testosterone (10.3%, p < 0.02).
Conclusions: In regards to performance, a strict KD seems to augment positive strength related adaptations when compared to a CKD. These responses may be explained by sustained total testosterone levels seen in the KD group compared to reductions in total testosterone as a result of the fluctuations in macronutrient intake.
Practical Applications: Individuals attempting to optimize adaptations in strength performance while maintaining testosterone levels should perform a KD compared to a CKD.
My take: no difference between KD & CKD, despite testosterone declining in CKD. This isn’t surprising because small fluctuations within the physiological range are not expected to affect these outcomes.
When protein and calories are controlled, and the #context is a 500 kcal deficit, not really sure what they were expecting. Because of the constant deficit, insulin will be low even on the carb-up days, and those carbs are more likely to be burned off than replenish glycogen.
Continue reading →