Interleukin-1 beta: produced by activated M1 macrophages, classical fever-inducing cytokine, mediates cellular inflammation, and induces COX-2 (target of NSAIDs). Also involved in autoimmunity. You don’t want none of it but you certainly don’t want a lot of it.
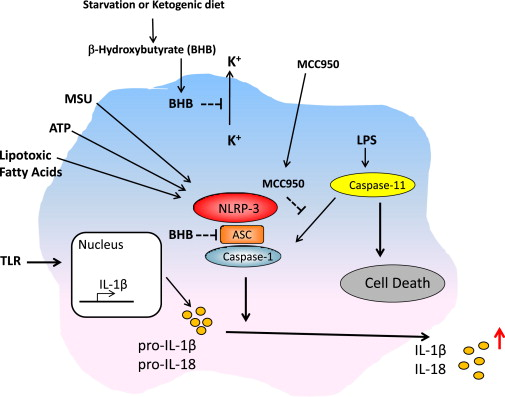
The ketone metabolite beta-hydroxybutyrate blocks NLRP3 inflammasone-mediated inflammatory disease (Youm et al., 2015)
This is a very specific effect: 1) many structurally similar compounds don’t block NLRP3; and 2) beta-hydroxybutyrate doesn’t block activation of other inflammasomes.
“In vivo, BHB or a ketogenic diet attenuates caspase-1 activation and IL-1b secretion in mouse models of NLRP3-mediated diseases such as Muckle-Wells syndrome, familial cold autoinflammatory syndrome and urate crystal-induced peritonitis. Our findings suggest that the anti-inflammatory effects of caloric restriction or ketogenic diets may be linked to BHB-mediated inhibition of the NLRP3 inflammasome.”